This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.This blog is done by 103.Pavan & 104.Jeshmitha
A 55yr old female resident of chityal with history of seizures
Chief complaints:-
The patient was brought to casuality with chief complaints of Active involuntary movements ,since 30 minutes, history of frothing from mouth deviation of eyeball upwards ,tongue bite with urinary incontinence no h/o of fever, head injury, vomitings, loose stools.
HISTORY OF PRESENTING ILLNESS:-
Patient was apparently asymptomatic 20 yrs back later she developed sudden onset of movements in upper and lower limbs for 5 minutes , confusion
The frequency & duration of episodes were gradually increasing with in these 20 years
Initially it was 1 episode in 5 yrs ---->later 2-3 episodes within 5yrs ----->one episode in 2years ---> single episode in 1yr ---->2-3 episode in a year
Last episode -
Current presentation -
on 1 dec she 5-6 episodes of seizures lasting for 10 mins,associated with confusion after the episode triggered by unilateral headache (30 mins prior to onset of symptoms), stiffening, sudden onset of involuntary movements, confusion uprolling of eyes, frothing, involuntary micturition. deviation of mouth towards left and postictal clouding.
H/o one episode of seizure activity after bringing to casualty
no h/o of involuntary defecation
no h/o fever, cough, vomitings, loose stools, pain in abdomen.
PAST HISTORY:-
K/C/O epilepsy since 20 years on medication not a known case of DM/HTN/TB/Asthma/CVD/CAD
TREATMENT HISTORY:-
On treatment for epilepsy since 20 yrs.

PERSONAL HISTORY:-
diet: mixed
Appetite: normal
sleep: adequate
bowel and bladder:normal
no addictions
FAMILY HISTORY:-
Not relevant
GENERAL EXAMINATION:-
Patient is drowsy not arousable
moderately built and nourished
Pallor - Absent

Icterus - Absent
Cyanosis - Absent
Clubbing - Absent
Lymphadenopathy - Absent
Pedal edema-absent
VITALS:-
Tempurature - 102.2 F
Pulse- 128 bpm
Blood pressure - 140/90 mmhg
Respiratory rate - 28 cpm
spo2- 94
grbs- 222mg/dl
SYSTEMIC EXAMINATION:-
CVS-
Inspection:-
JVP not seen
Auscultation
S1 S2 heard , no murmurs
RESPIRATORY SYSTEM
chest is bilaterally symmetrical
bilateral airway entry present
trachea - Midline
no scars
Percussion:-Resonant in nine quadrants
Auscultation- Normal vesicular breath sounds heard
ABDOMINAL EXAMINATION
shape- scaphoid
no tenderness
liver not palpable
spleen not palpable
CNS EXAMINATION
level of consiousness:- stuporous
speech- no response
Attitude and position - patient was lying on the bed in supine position
Bulk -




Rt. Lf
arm. 25 cm. 25cm
Forearm. 20cm. 20cm
Thigh. 35cm. 30cm
Leg. 28cm. 28cm
signs of meningeal irritation-
neck stiffness- no
kernigs sign-no
cranial nerve examination- cannot be elicited
motor system
sensory system- cannot be elicited
glassgow coma scale- E1 V1 M6
Pupils - reactive to light
Tone - Rt. Lf
UL. Normal. Normal
LL. Normal. Normal
Power Rt. Lf
UL. Absent. Absent
LL. Absent. Absent
Reflexes -
superficial reflexes
cornea- present
conjunctiva - present
Deep tendon reflexes-
Rt. Lt
Biceps: 2+ 2+
Triceps 2+. 2+
Supinator. 1+ 1+
Knee. 1+ 1+
Ankle absent. Absent
Cerebellar signs cannot be elicited.
gait- cannot be elicited
PROVISINAL DIAGNOSIS- GTCS secondary to acute CVA
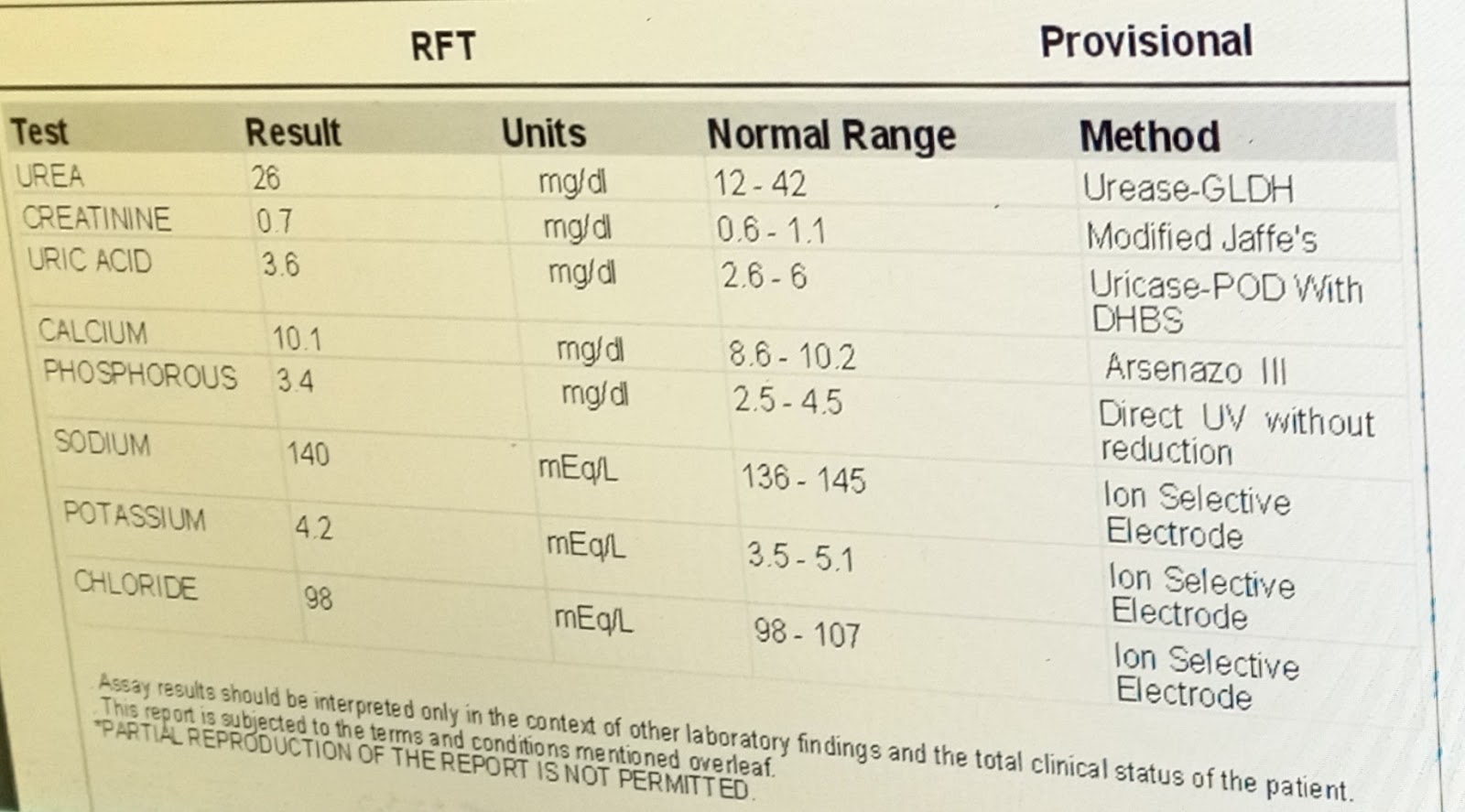
INVESTIGATIONS:- ON day1







TREATMENT :
She was given
Inj.loraz 2cc IV
Inj.Neomol 1gm
Inj.nevipil 2gm

Comments
Post a Comment